Hyperactive Bowel Sounds
Hyperactive Bowel Sounds Definition
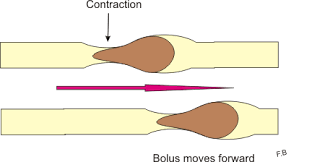
The motor functions of the stomach and small intestine are characterized by distinct manometric patterns of activity in the fasting and postprandial periods. The fasting is characterized by a cyclic motor peristalsis, the interdigestive migrating motor complex.
Mechanism of Bowel Sounds
In healthy individuals, one cycle of this complex is completed every 60 to 90 minutes. The complex has three phases: a period of quiescence, a period of intermittent pressure activity, and an activity front during which the stomach and small intestine contract at highest frequencies (3 per minute in the stomach, 12 per minute in the duodenum, 8 per minute in the ileum).
In the distal small intestine is the large migrating complex that empties residual content from the ileum into the colon in bolus transfers. (1)
During the process of digestion, the proximal stomach accommodates food by the reduction of its tonus. Thus. it facilitates the ingestion of food, whilst it does not increase the pressure.
It has been noted that half emptying time for non-solid food is approximately less than 20 minutes. Digestible food compounds are emptied after their size is less than 2 mm.
Hormone Role
There are several homones that regulate the motor and digestive process such as gastrin for acid secretion, cholecystokinin for gallbladder contraction and bile and pancreatic secretion. Insulin, glucagon and incretins regulate glucose homeostasis.
The small intestine is in charge of the transport of solid and liquids. It is known that liquids usually reach the colon before solids. Chyme is transported from ileum to colon intermittently in boluses. (2)
In the postprandial period, the interdigestive migrating motor complex is replaced by an irregular pattern of variable amplitude and frequency.
Vomiting is characterized by a sequence of motor events, including contractions of the stomach, abdominal muscles, and diaphragm.
Causes of Hyperactive Bowel Sounds
Colonic Motility
Basically, the healthy colon has short-duration (phasic) contraction. There are nonpropagated phasic contractions with the role in segemnting the colon into haustra. In that case, the action of mixing, retention or residue is facilitated, as well as the formation of solid stool.
In case of propagated contractions with high amplitudes (greater than 75 mmHg), propagation occurs over a distance of at least 15 cm.
Colonic transport of the content is a discontinuous process. Frequetnly, it may be slow or rapid. In certain cases, residues may be retained for prolonged periods in the right colon, A mass movement may bring the contents to the sigmoid colon in a few seconds. Feeding stimulates the movement of colon (gastrocolonic response).
In healthy individuals, the median transit period from oral cavity to cecum is about 6 hours. The same process through the right colon, left colon and sigmoid colon is about 12 hours each. In case of increased dietary fibers, average colonic transit time is decreased, stool frequency increases and stool consistency is softer. If there is a large amount of calories, the colonic transit is slower.
On average, nearly 9 liters of fluid enters the digestive system by oral intake and endogenous secretion.
Defecation And Continence
In order to perform a physiological defecation, it is necessary to obtain a series of coordinated actions of the colon, rectum, pelvic floor and anal sphincter muscles. The rectum is able to accomodate to a 300 mL prior a sense of fullness and urge to defecate.
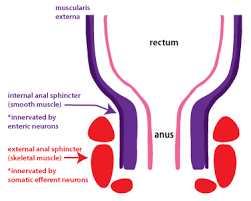
Distension of the rectum leads to the relaxation of the internal anal sphincter so called rectoanal inhibitory reflex and simultaneous contraction of the external anal sphincter to maintain continence.
The anal transition zone is able to sense the difference between solid or liquid stool and gas.
Disorder Of Transit Through Stomach And Small Bowel
Dumping Syndrome And Rapid Gastric Emptying
Dumping syndrome and rapid gastric emptying are common after truncal vagotomy and gastric drainage procedures. In case of highly selective vagotomy and antacid therapy, such conditions are less frequent.
In case of high calorie intake, insulin response is stimualted with consequent hypoglycemia. In these individuals, there is an impaired antral contractility and gastric stasis of solids that may lead to gastroparesis, in case of solid foods, and dumping, in case of liquids.
Rapid Transit Dysmotility
Rapid transit of solid food through the small bowel may be present in the irritable bowel syndrome, postvagotomy diarrhea, short bowel syndrome, diabetic diarrhea and carcinoid diarrhea.
The majority of these conditions lead to the onset of severe diarrhea with the significant loss of fluids and electrolyte disbalance. In case of idiopathic acid catharsis there may be present an inability of the distal ileum to reabsorb bile acids. There is also reduced contact time with the ileal mucosa. Such condition may lead to higher colonic secretion and secondary diarrhea. Such rapid transit of food may be confirmed by scintigraphic studies.
Diagnosis
The most common diagnostic approach is auscultation of the abdomen and bowel, vascular sounds and friction rubs.
Abdomen Auscultation. Image Source – Fotosearch.com
Normal sounds are present in case of physiological peristaltic activity. Peristalsis is characterized by progressive wavelike movements that occur involuntarily in hollow tubes in the abdomen. Inflammatiion of the intestinal mucosa will cause hyperactive bowel sounds. (3)
Treatment
Rehydration
Treatment is focused on the rehydratation and an adequate nutrition, as well as slowing down the bowel transit. Dietary interventions include the avoidance of hyperosmolar fluids and inclusion of isoosmolar or hypoosmolar oral rehydratation solutions. The fatty dietary components must be reduced to 50 g/day in order to avoid delivery of unabsorbed fat to the colon.
Electrolytes
The electrolyte and nutritional deficiencies minerals such as calcium, magnesium, potassium, and water and fat soluble vitamins should be corrected or supplemented.
In patients with less than 1 m of residual small bowel, it may be difficult to maintain fluid and electrolyte balance without parenteral support. In patients with a longer residual segment, oral nutrition, pharmacotherapy, and supplements are usually effective.(4)
Pharmacotherapy
- The opioid medication loperamide (4 mg 30 minutes before meals and at bedtime) suppresses the motor response to feeding and improves symptoms but may be ineffective or cause side effects (the most common is hypotension).
- Verapamil (40 mg twice per day) and/or clonidine (0.1 mg twice per day) may be used in addition to loperamide.
- Octreotide (50 μg subcutaneously three times per day before meals) may be used in patients for whom the oral agents are ineffective or poorly tolerated.
- 5-HT3 antagonists (alosetron) may be efficacious in the treatment of carcinoid diarrhea and diarrhea-predominant irritable bowel syndrome.
REFERENCES
- Linan-Rico A..Mechanosensory Signaling in Enterochromaffin Cells and 5-HT Release: Potential Implications for Gut Inflammation.Front Neurosci. 2016 Dec 19;10:564. doi: 10.3389/fnins.2016.00564. eCollection 2016.
- Ge X. Potential role of fecal microbiota from patients with slow transit constipation in the regulation of gastrointestinal motility.Sci Rep. 2017 Mar 27;7(1):441. doi: 10.1038/s41598-017-00612-y.
- Moll van Charante EP. Auscultation of the abdomen. Ned Tijdschr Geneeskd. 2011;155:A2657.
- Sánchez-Carpintero de la Vega M, García Villar C.Fluoroscopic studies of the upper gastrointestinal tract: techniques and indications. Radiologia. 2017 Jan 25. pii:


