Biliary Dyskinesia
What is Biliary Dyskinesia?
Biliary Dyskinesia is a medical disorder that occurs when the normal peristaltic mechanism of the gallbladder, the biliary tree and the sphincter of Oddi. In essence, it is simply a motility disorder where no underlying cause of the syndrome can be immediately elicited.
This is a misleading disorder as that this can be confused with the actual acute cholecystitis secondary to cholelithiasis or stones in the gallbladder. The latter is a formidable and critical disease on its own and requires emergent medical intervention in order to avoid potential devastating complications.
We will review the biliary system and its associated organs to get a glimpse of how biliary dyskinesia or better known as acalculous cholecystopathy occurs.
Pathophysiology & Causes
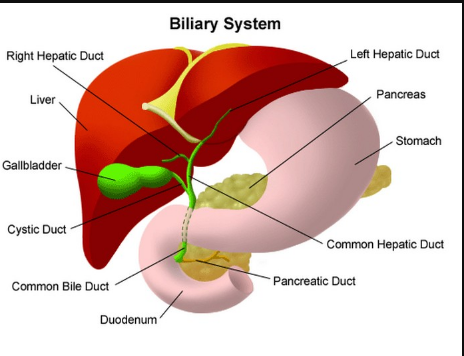
The biliary system which includes the liver, the bile duct, pancreas and gallbladder is responsible for release of bile salts responsible for aiding in the digestion and absorption of fats. In order for the biliary system to work in concert, there must be a coordinated signaling of hormones and stimuli that enable the secretion of much needed enzymes.
The liver continuously produces bile salts which trickle down from the liver down to the sphincter of Oddi which opens into the second part of the duodenum of the small intestines.
However, since the sphincter is normally closed when there is no meal the bile back flows into the gallbladder for storage and later release. Only when cholecystokinin is released that the gallbladder contracts and the sphincter opens and the force of gravity pulls the bile salts down to help in digesting fats.
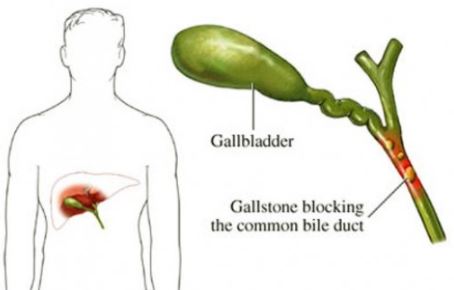
Unfortunately in cases wherein there is an acute obstruction of the lumen or anywhere down the biliary tree and a fatty meal is consumed, be it a stricture, a gallbladder stone, an infectious process or an Ascaris worm that makes it into the biliary tree, the gallbladder contracts against a blocked lumen, building up pressure and causing the distinctive right upper quadrant pain in acute cholecystitis.
If this continues, the bile will backflow into the gallbladder causing hydrops as well as finding its way back into the systemic circulation causing a yellowish discoloration of the body known as jaundice. To confirm the presence of acute cholecystitis secondary to gallbladder stones, a good history is extracted from the patient that usually includes risk factors such as middle age, overweight and more often female.
Lab tests are done to verify if the source is a blockage by measuring direct bilirubin levels. Afterwards, a radiologic examination in the form of an abdominal ultrasound will detect the presence of stones in the gallbladder. This is the usual schema in biliary tree diseases and the treatment of choice is usually finding the source of the blockage and removing it.
In biliary dyskinesia however, there is no actual obstruction and it’s more of an impairment of the usual motility of the biliary tree in response to a fatty meal. There are many studies that aim to explain the reason why there is a slowing of the peristaltic movement of the biliary tree.
Some drugs such as Calcium channel blockers, octreotide, progesterone, indomethacin, theophylline, benzodiazepines and histamine blockers are known to slow the motility of the biliary tree.
One possible explanation for the slowing of peristaltic movements is the constant intake of fatty food that forces the gallbladder to contract continuously that eventually wears down the ability of the biliary tree to contract effectively. This also is apparent in old age where most body functions are decreased and are unable to keep up with the demands of food digestion and absorption.
Symptoms
The patient usually presents with right upper quadrant pain which may or may not have tenderness, varying degrees of leukocytosis, fever and elevated liver enzymes unlike that of the usual cholecystitis with gallstones. To diagnose this, gallbladder ejection fraction is measured. If the ejection fraction is less than 40% then the patient is at high risk for biliary dyskinesia, treatment may be needed in the form of surgery.
Treatment
Currently there are no effective treatments against biliary dyskinesia, however surgical treatments via laparoscopic cholecystectomy research result into symptomatic relief in over 96% of patients versus those that were managed with only medical therapy. Complications of surgery are similar to that of calculous cholecystitis.
Bleeding, infection and damage to nearby structures of the biliary tree are potential complications and rate of bile duct injury is about 3 in 1000 procedures. Other new developments in the field of treating biliary dyskinesia are targeting the sphincter of Oddi.
This disorder of Oddi has two types; the one affecting just the biliary outlet and the other one affecting the pancreatic outlet. Patients with the biliary type typically present pain 4-5 years after a cholecystectomy. A manometry may be performed to assess its functional capabilities. Sphincterectomy may be performed and is known to cause relief in 80% of patients.
Conclusion
Biliary dyskinesia is certainly one of the greatest challenges that physicians have today. The presence of the usual signs and symptoms of acute cholelithiasis with no actual stone on ultrasonography may prove a challenge to explain to the patient the option of surgery to treat its signs and symptoms. But whatever the challenges maybe, research into the near future about the biliary tree and how it works will provide us with a good way to improve our healthcare practices for better outcomes.


